Dr. Ryan Hsi
Kidney Stone Disease Specialist
BOOK APPOINTMENT

Meet
Dr. Ryan Hsi
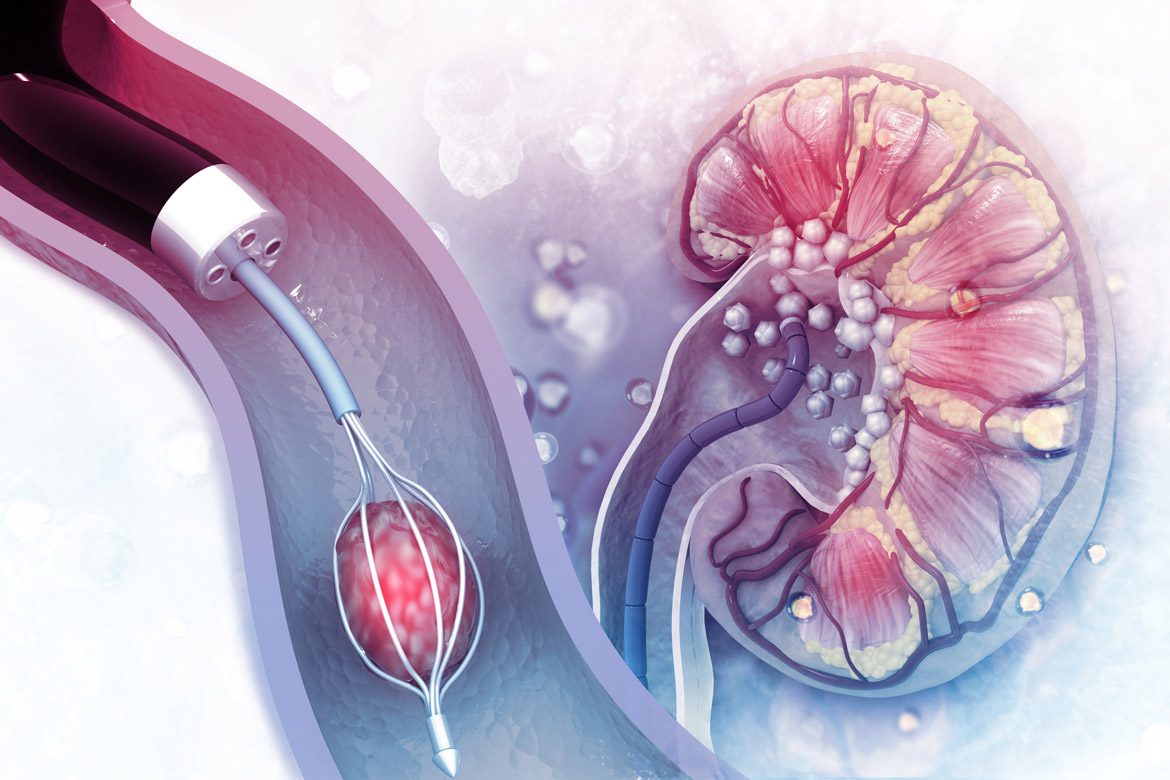
Dr. Ryan Hsi is an endourology and kidney disease specialist in Orange County, CA, and a nationally recognized expert in kidney stone disease. He specializes in minimally invasive and endourologic surgery, offering advanced treatments such as ureteroscopy, laser lithotripsy, and mini and standard percutaneous nephrolithotomy (PCNL).
Dr. Hsi’s research focuses on improving the prevention, diagnosis, and management of complex kidney stones through clinical trials, health services research, and data-driven innovations.